Tesla has been gladly laying off its workers, while bemoaning a massive loss of IKEA mugs, and yet investing heavily into what looks like a mysogynist “torture room“.
Elon Musk seems to have built a ‘mega rave cave’…
Andre Thierig, a senior manufacturing director at the factory, shared a LinkedIn post about the new space called Hamster.
“Say hello to our newest ‘facility’ at Giga Berlin! Hamster is now alive,” he said in the post. “Do you know any factory that has its own club? Party on!”
The man associated with Epstein, who is running this project, allegedly called it his Hamster room because… thinly veiled references to targeted abuse and exploitation of women still are not well known outside of systemic rape culture.
The Manosphere contains many, many words regarding a woman’s rationalization hamster because it’s such an effective and amusing way to describe how a woman thinks. […] When the hamster rationalizes successfully, a woman can divorce [yeah, I meant to use that verb] herself from the consequences of her bad decision or behavior.
The Hamster room. It means rape, as Peter Thiel explained in his book.
…there’s a line in the book that describes, you know, rape – date rape as, you know, seductions later regretted…
Tesla has announced a literal “full-throat MAGA” rape cave, as a monument to toxic work culture built at great expense while staff are being fired due to a collapse in sales.
What will Tesla toxic management think of next for their German factory, an automatic weapon shooting range called “Hit her”?
As reported by the BBC in February, former Prime Minister (PM) Liz Truss said it’s time for violence:
…conservatives are now operating in a hostile environment… we essentially need a bigger bazooka in order to be able to deliver…
Truss, the shortest-term PM in the United Kingdom’s (UK) history and the first ex-PM to completely lose any seat in government (due to extreme incompetence), was a featured speaker at the Conservative Political Action Conference (CPAC).
Given her outlandish calls for domestic terrorism and civil war, as a literal nobody in America who can still seriously damage the political narrative, now she has been invited as an honored guest to the Republican National Convention (RNC).
‘I don’t know who that is’: What Americans think of Truss at Republican convention
Not knowing who she is makes her big stage speech calling for US violence even more dangerous, as it enters the dialogue with authority yet without real attribution.
Seven in ten UK voters have an unfavourable view of Trump – even more than have an unfavourable view of Truss.
Trump is shamelessly using Truss. And you would think Americans could bounce Trump out of office faster than Truss, given he’s worse. Alas.
Obvious game-playing by the RNC to use a disgraced UK PM to stoke violent hate without attribution recalls dangerous Trump rhetoric that called for assassination of his political opponents.
Trump: If Clinton picks judges, “nothing you can do, folks — although the 2nd Amendment people, maybe there is.” […] Sen. Chris Murphy, D-CT, responded on Twitter: “Don’t treat this as a political misstep. It’s an assassination threat, seriously upping the possibility of a national tragedy & crisis.”
Trump responded to loud criticism of his obviously divisive call for assassination by invoking gaslighting propaganda tactics.
It’s called the power of unification…
By “it” he meant assassination. Trump openly called “it” his theory for unification, nudge, nudge, wink, wink, because he believes that killing his opponent… unifies power into him.
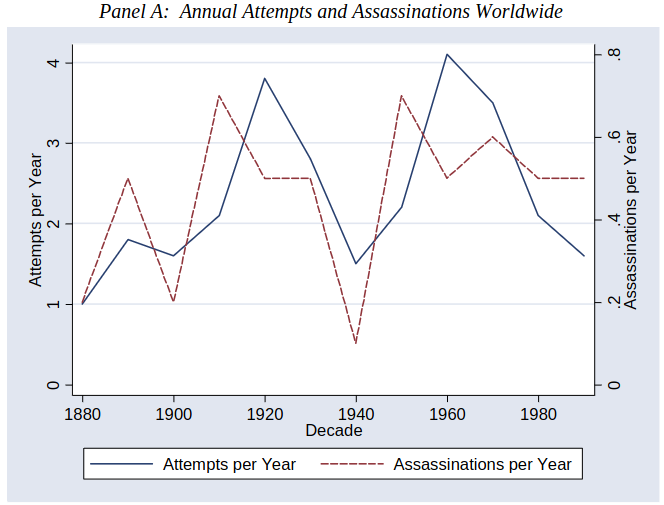
Source: “Hit or Miss? The Effect of Assassinations on Institutions and War”, by Benjamin F. Jones and Benjamin A. Olken, Northwestern and MIT, 2001
The GOP regular incitements to violence have now adopted this “unity” phrasing along with some of their more obvious incitements.
In Ohio campaign rally, Trump says there will be a “bloodbath” if he loses November election…
How could they so horribly misuse the word “unity” to campaign for violent disunity in America?
First, don’t discount how calls for unity towards preserving slavery were the defining feature of racist Confederacy secession. White men were tortured and lynched, their mutilated bodies strung up in public displays, if they dared to object to American prosperity being based almost entirely on mass human trafficking. Unity was demanded to prop up the systemic government-sanctioned rape of Black women for profit, with even anti-racist speech facing penalty of gruesome public death by mobs.
John Brown grew tired of torture and murder of abolitionists and called for armed defense against violent “unity” demanded by slavery. Curry’s “Tragic Prelude” impressive mural can be seen in the Kansas State Capitol celebrating his moral conviction to defend Americans against tyranny.
Second, the modern answer is the GOP have shifted their messaging hard towards a well-known reverse meaning used by current domestic terrorists, an encoded white supremacist signal related to extremist “replacement” racist conspiracies.
White Supremacist Propaganda Incidents Soar to Record High in 2023… common slogans include “White unity”…
Notably, at public rallies they leave the “white” part out like they leave their white hoods off.
Unity has been a theme of the Republican convention this week in Milwaukee…
Thus unification through hate, and especially violent hate, is a very old theme in American politics.
“[The organized terror movement after Civil War] stock-in-trade was violence – intimidation and violence. People were beaten, people were flogged, people were lynched, people were shot. People’s homes were raided, they were dragged outdoors and flogged in the streets.” And, he says, the violence often included “truly horrifying sadism”.
…a former Ku Klux Klan leader and a current U.S. Senate candidate from Louisiana — encouraged listeners to cast their ballots for Trump, saying that “voting against Donald Trump at this point is really treason to your heritage.”
Colby: On the 29th of October 1869, [the KKK] broke my door open, took me out of bed, took me to the woods and whipped me three hours or more and left me for dead. They said to me, “Do you think you will ever vote another damned Radical ticket?” I said, “If there was an election tomorrow, I would vote the Radical ticket.” They set in and whipped me a thousand licks more, with sticks and straps that had buckles on the ends of them.
Source: Encyclopedia of Alabama, 1 Sept 1868 Tuscaloosa Independent Monitor. The KKK threatened that on March 4, 1869 — the first day of rule by avowed racist Horatio Seymour — would bring lynchings of white Americans (“scalawags” and “carpetbaggers”) who had voted against him. Instead the Presidency was won in a landslide by Civil War hero and civil rights pioneer Ulysses S. Grant)
The brand of bazooka-driven (assassination, bloodbath) “unity” the GOP is talking about is simply white supremacist violence, an 1800s-themed war to put white men into power and remove everyone else.
Not only has Tesla failed to deliver a safe vehicle as promised, there’s evidence it’s making roads exponentially less safe for everyone… and especially Tesla owners.
Source: Commerce City Police Department
Two Teslas crashed in Commerce City on Wednesday, sending both drivers to the hospital. According to the Commerce City Police Department, the crash occurred at Landmark Drive and 104th Avenue intersection. The intersection is largely residential, east of Second Creek Open Space and Chambers Road.
While the Tesla CEO often falsely claims his cars have “collision avoidance”, crashes like this prove nobody should be buying his lies.
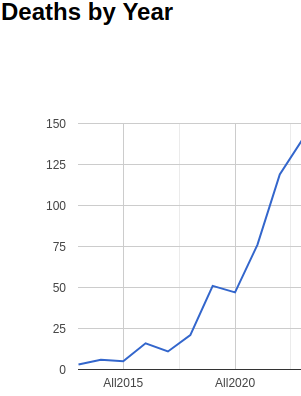
The company didn’t speculate on how much [their January 2017 press] release might improve safety, but Musk said that the final effect would be massive. “Our target is a 90 percent reduction [in crashes] as the software matures,” he posted on Twitter.
He said 90 percent only because it sounds really good to investors, not in any way basing such stock-pumping claims on facts about actual crashes. And since 2017 what has happened? Tesla safety plummeted, deaths and injuries rocketed.
The Trump hate campaign has dialed up the stakes, promising supporters to remove all Blacks and Hispanics from government positions. They’ve just selected one of the most wealthy notoriously “anti-poor” racists as VP.
…staunch Trump supporter who has promoted the “Great Replacement Theory” which is rooted solely in racism. […] “It’s not just that Donald Trump doesn’t speak to issues of special concern of minority voters or Black voters, it’s that he seems to like actively antagonizing a lot of the Black voters,” Vance stated on CNN…
Trained in the U.S. Marines as a military “journalist” disinformation expert who then attended Ivy-League school, J.D. Vance took a plumb appointment in Peter Thiel’s infamous anti-democratic venture firm.
Is it any wonder why Vance since then has been campaigning for a cushy non-job to undermine democracy and bring Nazism back, while he notoriously engages in dangerous racist propaganda?
Five experts on hate speech who reviewed [Vance’s] comments confirmed that they promote the baseless racist theory, even though the Republicans don’t mention race directly. […] In Ohio, Vance has already secured a place on the November ballot. He won Trump’s endorsement after embracing many of the former president’s hardline views, including those related to immigration.
That’s a trained military propagandist for you. Spreads racism while claiming to never have used the exact word, as if that’s a defense.
The only time Vance explicitly mentions racism is to accuse others of it, or to claim he can’t possibly be a racist because he married a wealthy Asian woman (he met at Yale) and thus describes his children non-white and his wife not-Christian.
In 2013, he and Usha organised a discussion group on “social decline in white America”…
His wife made her money fighting against Title IX claims in California (rape, sexual assault, sexual battery, and sexual coercion) and clerking for Judge Brett Kavanaugh (credibly accused by multiple women of sexual assault).
Needless to say, his protests never seem to land on wanting to be an anti-racist, instead only viscously accuse others of being the racists. He claims white replacement theory is just him wanting to build a wall, like saying Auschwitz was just Hitler wanting to build a fence.
That’s a trained military propagandist for you. In other words Vance, who wrote a best-selling book to slander successful American Blacks as “aliens“, was literally chosen by Trump as an encoded white supremacist voice to antagonize Black voters.
Even worse, Vance literally admired Trump as an equivalent to Hitler before accepting the VP position.
Vance previously called [Trump] an “idiot”, “noxious” and “reprehensible”… “America’s Hitler”.
…the former president said at a rally that Vance was “in love with me” and “kissing my ass.”
What better way for Vance to get on the hate ticket than to regularly unleash so much hate?
Clearly the Vance pick means extremist hate. America has seen this before many times, as Presidential campaigns often have been extremely racist (e.g. Jackson, Seymour, Wilson, Nixon, Reagan, Trump).
After Grant crushed the KKK political platform in 1870s, it rebranded itself a Christian nationalist “America First” platform in 1880s to encode the same racism in Presidential campaigns.
Already the U.S. is seen abroad as under threat from hate groups, much like in 1933 when the Hearst empire tried to put pro-Hitler candidates into government.
Trump’s running mate JD Vance has insulted the UK with his racist ignorance.
Trump and Vance, fraudulent elitists, are running for office on a hateful “let white man rule” ticket like the Civil War never ended.
a blog about the poetry of information security, since 1995